Wednesday, February 17, 2016
qotd: Medicare's History Belies Claim That Medicare-for-All Would Disrupt Care
The Huffington Post
February 16, 2016
Medicare's History Belies Claim That Medicare-for-All Would Disrupt Care
By Steffie Woolhandler and David Himmelstein
ASSOCIATED PRESS
*It Disrupted Jim Crow, but Otherwise the Transition Was Smooth*
Hillary Clinton and others charge that Bernie Sanders' Medicare-for-All
plan would disrupt and threaten Americans' health care. But the smooth
rollout of Medicare-for-Seniors in 1965 -- which many had also predicted
would bring chaos -- belies that charge.
Medicare, signed into law on July 30, 1965, went live just 11 months
later. By then, 18.9 million seniors had signed up, 99 percent of those
eligible.
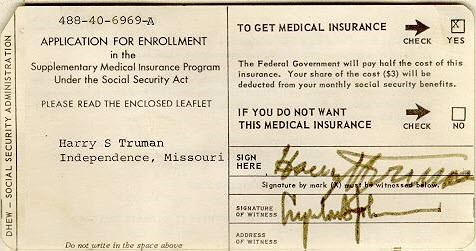
To accomplish this feat (largely without computers) the Social Security
Administration mailed an information leaflet and sign-up cards
<https://www.ssa.gov/history/ssa/lbjmedicare3.html> preprinted with each
individual's name and Social Security number (see example below) to
seniors on the Social Security and railroad retirement rolls, as well as
Civil Service annuitants and a million other seniors identified through
IRS records.
2016-02-16-1455651003-9836566-Medicareenrollmentcard.jpg
<http://images.huffingtonpost.com/2016-02-16-1455651003-9836566-Medicareenrollmentcard.jpg>
{kind=link}
Image: Social Security Administration History Archives
To contact hard-to-reach seniors, the federal government reached out to
nursing and retirement homes, employers, unions and civic organizations
offering to help people apply; organized hundreds of local information
meetings; and enlisted postal workers, forest rangers and agricultural
representatives to help locate residents of remote areas. The Office for
Economic Opportunity hired 5,000 low-income seniors who went
door-to-door in their neighborhoods.
All told, Medicare's overhead costs for the first year totaled only $120
million (equivalent to $882 million in 2015). By comparison, setting up
the insurance exchanges for private coverage under Obamacare cost more
than $6 billion
<http://healthaffairs.org/blog/2014/01/02/medicares-rollout-vs-obamacares-glitches-brew/> --
about seven times as much. But even the modest figure for Medicare's
start-up costs is an overstatement since it includes the cost of
processing six months' worth of medical bills, not just the enrollment
costs. Moreover, Medicare and Medicaid (which was passed at the same
time) displaced several smaller federal health assistance programs,
saving about $383 million (in 2015 dollars) on their overhead costs.
Even as it became clear that Medicare enrollment was proceeding
smoothly, many saw disruption ahead. The Association of American
Physicians and Surgeons (AAPS), a group to the right of the American
Medical Association (AMA), threatened that 50,000 doctors would boycott
Medicare. (Today, the AAPS is sounding the alarm that Medicare-for-All
would take away "what remains of your doctor's liberty.") Wall Street
Journal headlines warned that "Most MDs Won't Cooperate," and foresaw a
"Patient Pileup," as "flocks of Medicare beneficiaries ... suddenly clog
the nation's 7,200 hospitals."
None of this came to pass. Doctors continued to care for elderly
patients, mostly accepted Medicare payment, and soon came to rely on
Medicare as an economic pillar of their practices. Even the AMA, which
had spent millions fighting Medicare's passage (including an infamous ad
campaign <https://www.youtube.com/watch?v=Bejdhs3jGyw> featuring
then-actor Ronald Reagan) cooperated in the program's implementation.
Hospitals ran smoothly, with only a handful reporting more than minor of
problems.
But Medicare did cause a major disruption, it disrupted Jim Crow
hospital care.
The 1964 Civil Rights Act banned racial discrimination in facilities
receiving federal funds (which included most hospitals), but enforcement
was lax until Medicare.
<http://www.hhnmag.com/articles/4179-u-s-hospitals-and-the-civil-rights-act-of-1964>Many
hospitals, particularly in the South, still refused to care for black
patients at all, while others relegated them to separate entrances and
shabby basement wards. Black physicians were often barred from hospital
staffs, and in many locales ambulance services were separate, and
distinctly unequal.
With Medicare on the horizon, federal officials made it clear to
hospitals that segregated hospitals would be excluded from the program.
In the spring of 1966, three months before Medicare took effect, 51
percent of American hospitals were still segregated. By August of that
year, 99.5 percent had desegregated.
While Medicare ended overt racial segregation in hospitals, segregation
by insurance remains legal and common -- and often perpetrates de facto
racial segregation. Most of New York City's prestigious academic medical
centers -- and many hospitals elsewhere -- maintain separate clinic
systems
<http://digitalcommons.law.umaryland.edu/cgi/viewcontent.cgi?article=1113&context=jhclp>,
and even separate wards, for Medicaid patients (the 33 million uninsured
need not apply).
Medicare-for-All would give all Americans complete and equal coverage,
completing the disruption of hospital segregation that Medicare began a
half century ago.
Aside from that welcome disruption, Medicare-for-All would greatly
simplify life for hospitals and doctors. Instead of the laborious and
expensive task of billing patients and their insurers for each Band-Aid
and aspirin tablet, hospitals would receive a lump-sum budget, much as
we pay for a fire station. Doctors would bill one plan, using one
billing form instead of the dozens of complex billing schemes -- each
with its own rules and redundant documentation requirements -- that we
face today.
Most important, Medicare-for-All would end many of the disruptions that
our patchwork coverage system currently inflicts on patients. All
Americans would, for the first time enjoy a free choice of doctor and
hospital, and would never again be forced to change doctors merely
because their insurance changed, or their doctor was dumped from their
insurer's network. And patients' lives would no longer be disrupted by
financial ruin from medical bills
<http://www.pnhp.org/new_bankruptcy_study/Bankruptcy-2009.pdf>.
/Drs. Steffie Woolhandler and David U. Himmelstein, professors of health
policy and management at the City University of New York School of
Public Health at Hunter College and Lecturers in Medicine at Harvard
Medical School, co-founded Physicians for a National Health Program, a
nonpartisan organization. The opinions expressed do not necessarily
reflect those organizations'./
Comment by Don McCanne:
"Nuf said. Time for Medicare-for-All.
Subscribe to:
Post Comments (Atom)
No comments:
Post a Comment